Advanced ‘toolkit’ for quality optimization in mammography
April 07, 2022
By Elina Samara, PhD, Medical radiation physicist, Valais Hospital, Switzerland
Breast cancer is the most frequent cancer among women and accounts for about 25% of all cancer cases and 15% of all cancer deaths (1). Especially in the European Union, it accounts for 29% of female cancer (2). Mammography is the basic imaging examination used to detect changes in the breast tissue, diagnose and manage patients with breast disorders. It is performed to both asymptomatic (screening mammography) and symptomatic patients (diagnostic mammography). Screening mammography is of particular interest in terms of radiation protection as asymptomatic individuals are exposed to radiation. Thus, optimized protocols are of crucial importance in mammography. One of the main advantages of a dose management system is that it offers a broad and direct overview of the radiological settings and practice (1). Parameters affecting the quality of the examination can be easily evaluated and optimization can be initiated based on facts.
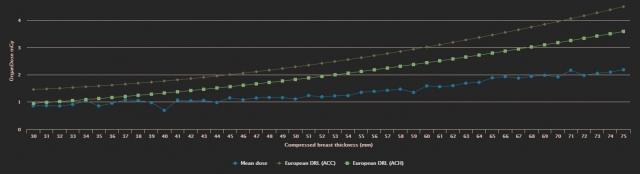
Diagnostic reference levels (DRL) have proven to be a practical tool widely used for patient dose optimization (3). The latest ICRP publication on the use of DRLs in medical imaging recommends the Mean Glandular Dose (MGD) as the DRL quantity to reflect the influence of different anode/filter combinations and breast thicknesses on radiation dose, which is not possible with other quantities (entrance surface air kerma free-in-air or entrance skin dose) (3). DOSE by Qaelum (DOSE) allows for exposure analysis taking into account the breast thickness and the reference values. We identified that local values were much lower than the reference ones (Figure 1), and thus, we defined new, local levels for diagnostic and screening examinations in order to better optimize exposure (1).
Figure 1: Comparison of mean MGD for screening mammography (y-axis, measured in mGy) with European DRL for different breast thicknesses (hospital mean MGD values are displayed as blue dots, while achievable and acceptable European MGD values are shown with green squares and brown rhombuses, respectively)
Alongside the analysis of separate radiological units, DOSE provides advanced comparison of MGD on our three different centers (figure 2). The number of screening examinations performed during the last two months was 267, 47 and 162 for the three centers respectively. Besides the wider distribution of doses that was noticed on 2 devices, it was observed that a number of patients received particularly high doses. By investigating these dose outliers further, we confirmed that they were associated with bigger breast thicknesses, so no correction actions were required.
Figure 2: MGD comparison among three centers (screenshot from DOSE software by Qaelum, using the white background)
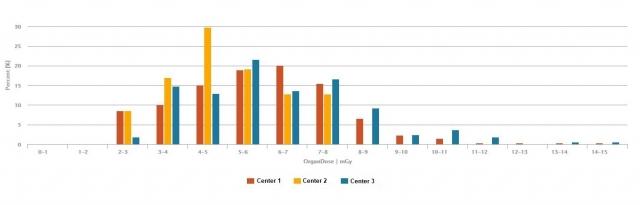
It is also interesting to note that the difference of dose distribution between the devices could be attributed to the different filtration used. Indeed, the mammography unit installed in center 2 is of older generation and lacks a filter installed in the other two. All these details could be found through the dose management system.
Estimating the dose in radiological practice is of major importance as it is linked to the radiation risk, yet not the only parameter to evaluate. Specific to mammography, the compression applied to the breast has a direct impact on both image quality and dose.
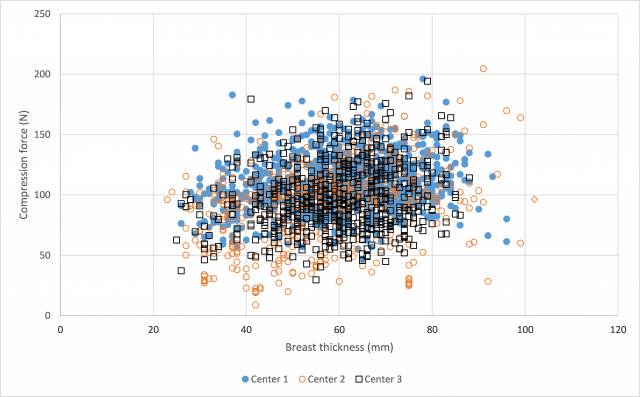
Radiographers need special training to correctly position the patient and apply the necessary compression that allows optimal image quality and exposure parameters. This data is analyzed in DOSE and can also be exported if needed. Figure 2 shows the applied compression force versus breast thickness. The general guideline followed in our hospital is to apply a compression force of 100 N (1). In center 1, radiographers applied significantly higher compression force (110 N) than the other two (93 N and 97 N) (p-value<0.001, figure 3). Although there were no complaints for image quality, the findings were presented and discussed with the radiographers to optimize their practice.
Figure 3: Compression force with breast thickness in 3 centers (Excel figure based on data exported from DOSE)
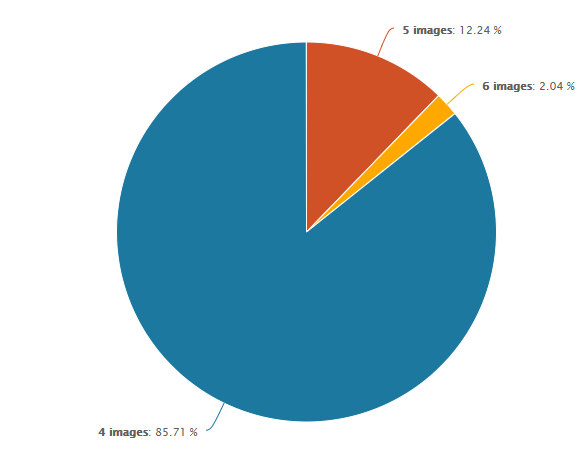
Another interesting finding is the number of images included in each exam. When talking about a mammography examination, it is usually considered having 4 images (bilateral craniocaudal and mediolateral oblique view images of left and right breast), which is not always the case (figure 4). DOSE allows a more thorough analysis to identify how many images are performed per examination as well as tracking the examinations that contain more images than usual. Rejected images may signify that radiographers need training, but often, clinical conditions such as big breast size require more than one images, which was confirmed in our case.
Figure 4: Number of images acquired for screening mammography (screenshot from DOSE software by Qaelum, using the white background)
DOSE is used as quality control tool for monitoring patient exposure under real conditions, checking compliance with DRL and detecting erroneous practice. Its integration to our institution allows us to have comprehensive overview and analysis of a significant amount of data for the performed radiological examinations.
References
- Samara ET, Tsapaki V, Sramek D, Dose management software implementation in mammography, Phys Med. 2019 Dec;68:88-95
- European Commission. ECIS – European Cancer Information System. https://ecis.jrc.ec.europa.eu
- ICRP 2017 Recommendations of the international commission on radiological protection ICRP Publication 135 Ann. ICR 46 (1)
Solutions
![]()
![]()
![]()
![]()
![]()
![]()
![]()



