Reducing Peak Skin Dose on patients undergoing interventional procedures
February 10, 2016
Interventional radiology is the radiology subdomain comprising minimally-invasive image-guided procedures for diagnosis and treatment purposes. It uses x-rays to guide small instruments such as catheters through blood vessels or other pathways in the body. Generally, the use of radiation is limited to a short time intermittently between manipulations of the needle, catheter, or probe. Nevertheless, the radiation doses after such interventions are often high.
Skin reactions typically occur after a certain radiation dose threshold. Therefore the goal is to keep Peak Skin Dose (PSD) as low as possible in order to potentially prevent severe clinical skin reactions and speed up (partial) skin recovery (Figure 1).
In this blogpost we focus on a number of aspects that may reduce radiation peaks on local skin areas and underlying tissues of patients.
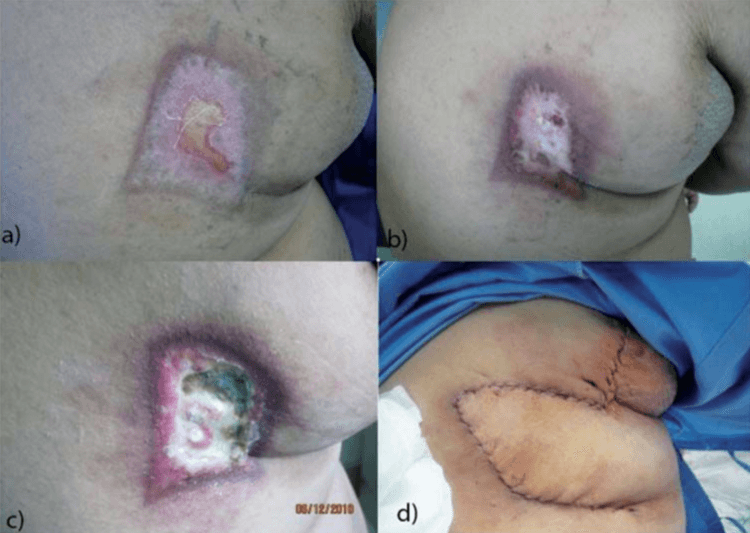
Figure 1. Skin injury (necrosis and ulceration) in a patient with chronic total occlusion. a) 2 months, b) 6 months, c) 8 months after percutaneous coronary intervention (PCI), and d) after the flap surgery. [pictures from: REHANI, M.M., SRIMAHACHOTA, S., Skin injuries in interventional procedures. Radiat. Prot. Dosimetry (2011); 147(1-2): 8-12, doi: 10.1093/rpd/ncr257].
Obviously the size of the radiation field is of great importance, but that is selected in function of the required imaging area during the interventional procedure. In general the distance from the patient to the x-ray tube is a measure for the amount of radiation the patient is exposed to. When feasible in light of the planned procedure, moving the table away from the x-ray tube and closer to the detector, decreases the radiation dose. Furthermore the degree of magnification and the different fluoroscopy modes (continuous/pulsed) applied, also play a crucial role as far as the patient’s dose is concerned.
Using multiple beam angles may also have a profound impact on reducing the radiation dose on the patient’s skin. By shifting the primary angle of the x-ray tube (RAO – LAO direction) to +20 and -20 degrees relative to home position (0 degrees), for example, the x-rays no longer exclusively penetrate the same area of the skin. Although a larger skin area gets exposed, the approach reduces PSD significantly (Figure 2). In addition, the operator may further exploit this favorable effect by varying the secondary angle (CRAnial-CAUdal direction).

1 angle (left image) – 3 angles (middle image) – 5 angles (right image)
Figure 2. Peak Skin Dose (PSD) illustrated using greyscale: from black (zero skin dose) up to white (maximum skin dose). The successive images show the change in PSD and skin area exposed when changing the beam angulation. The first image (white square) corresponds to the case where the tube is continuously irradiating in a single direction. When shifting the primary angle of the x-ray tube between -20 and +20 degrees relative to the home position (0 degrees), for example, the exposed skin area extends but the PSD decreases (light grey bars). When irradiating under more different angles, ranging between -40 to +40 degrees (with 20 degrees step size), PSD decreases significantly (5 angles case). The PSD area is now limited to a few narrow grey bars, which are caused by field overlapping.
The detailed effect of beam angulation is illustrated by the PSD analysis in DOSE, as shown below (Figure 3). From the start, PSD gradually increases almost linearly with the Dose at Reference Point (RP) (upper-left chart). The tube angle analysis chart (lower-left) shows that with the beam direction shifting frequently, it is possible to keep the PSD constant while the irradiation continues.

Figure 3. PSD increases together with the Cumulative Dose at Reference Point (RP) (upper-left chart). When the procedure is nearly half way, the beam angulation starts changing frequently (lower-left chart). As a result, PSD stops increasing even though the irradiation continues. This is illustrated by the ratio of PSD to Dose at RP that decreases (upper-right chart). This effect would not be assigned to beam angulation if the table was not almost stable during the procedure (lower-right chart).
The graphic below (Figure 4) illustrates two cases for which DOSE estimated the maximum skin dose and generated a dose distribution map. The comparison of these cases stands to the fact that most of the parameters are almost the same, yet the PSD differs significantly. From the angle analysis, it is noticed that one of the main differences was the number of beam angles used, as well as their frequency of use.

Figure 4. PSD map and angular dependency analysis calculated by DOSE, for (1) an 86-year-old and (2) a 60-year-old, both male patients, undergoing coronary catheterisation.
For both cases, the number of events is the same (75 events) and the Dose Area Product (DAP) value is almost equal (approx. 2300 dGy*cm2). However, PSD for patient 1 is 3.8 Gy, while for patient 2 is 1.4 Gy. In the case of patient 1 only a few beam angles are applied (lower-left chart), of which one specific angle is used for almost 80% of the procedure (red color approx. 60 events). On the contrary, in the case of patient 2, many beam angles are applied (lower-right chart) and in a more uniform frequency. That means that none of the angles is used for more than 35% of the procedure (green-yellow color), corresponding to only 26 events or less.
When orange or red pixels appear on the map, the dose is medium or high, depending on the severity of skin reactions it may potentially cause. In this case, a notification is generated to inform the user. At the same moment, a summary containing the skin and hair effects as a function of dose and related approximate time of onset of effects, is provided. DOSE even allows the automatic sending of an email or sms to the performing physician and/or relevant specialist, so that they can take immediate action and advise the patient.
Predicting or evaluating the amount of radiation the skin of a patient gets exposed to (during an interventional procedure) is not always straightforward. Therefore, interventionalists use DOSE by Qaelum to acquire an overview of the skin dose analysis after each procedure. Moreover, they use DOSE to analyse similar interventional procedures, and assess the relationships between PSD and the individual influencing aspects briefly discussed above. This way, they can identify techniques that require corrective actions in order to further increase patient safety.
For a more detailed analysis on this topic, we kindly refer to a poster presentation from the Qaelum team on the ECR 2016, entitled “Correlation of peak skin dose with geometrical and dosimetric parameters from interventional procedures” (C-1835).
Contact us for an in-depth demo and learn how you can start optimizing your interventional procedures today!
References
Skin injuries: Occurrence and Evolution (Radiation Protection of Patients – IAEA)
10 Pearls: Radiation protection of patients in fluoroscopy (Radiation Protection of Patients – IAEA)
Avoidance of Radiation Injuries from Medical Interventional Procedures: International Commission on Radiological Protection – ICRP)
http://www.icrp.org/publication.asp?id=ICRP%20Publication%2085
Skin injuries in interventional procedures, Madan Rehani, PhD, Radiation Protection of Patients Unit, IAEA
http://indico.ictp.it/event/a12208/session/38/contribution/24/material/0/0.pdf
Fluoroscopically Guided Interventional Procedures: A Review of Radiation Effects on
Patients’ Skin and Hair (Radiological Society of North America – RSNA)
http://pubs.rsna.org/doi/pdf/10.1148/radiol.2542082312
Guidelines for Patient Radiation Dose Management (Society of Interventional Radiology – SIR)
http://www.sirweb.org/clinical/cpg/Patient_Radiation_Dose_Management_Stecker.pdf
Skin injuries in interventional procedures (Rehani MM1, Srimahachota S., National Library of Medicine – NLM)
Solutions
![]()
![]()
![]()
![]()
![]()
![]()
![]()



